Population Gap Detector: AI Tool for Research Gap Analysis
Detect underrepresented populations and subgroup evidence gaps in biomedical research with AIPOCH's Population Gap Detector — a free, open-source AI agent skill on GitHub.
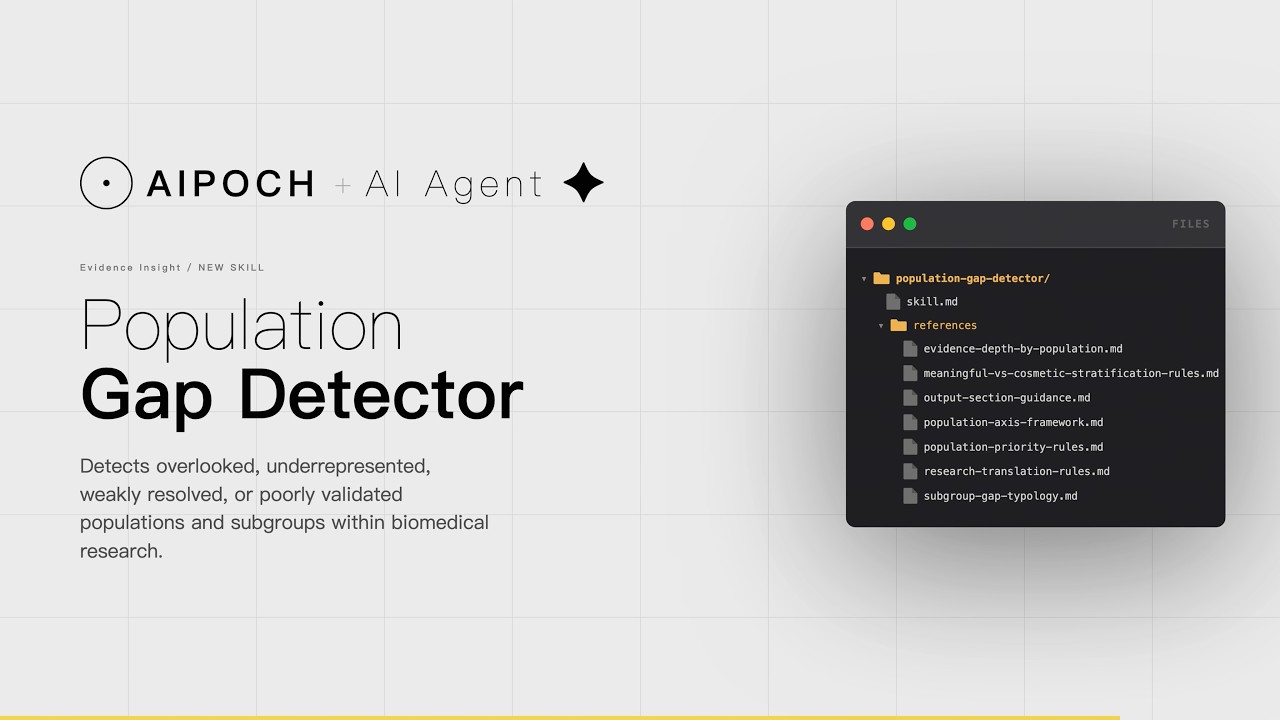
Identifying which populations are missing from a research area before designing a study is one of the most time-consuming and judgment-intensive tasks in biomedical research. The Population Gap Detector — a Medical Research Agent Skill from AIPOCH — is designed to support researchers in detecting overlooked, underrepresented, weakly resolved, or poorly validated populations and subgroups within a biomedical research area, so Researchers can identify more precise and meaningful study populations.
Population Gap Detector skill source and reference modules are openly available on GitHub: aipoch/medical-research-skills — population-gap-detector.
This article describes how the skill works, what kind of outputs it can help produce for researcher review, and the research workflow problem it is designed to address.
Why Identifying Population Gaps Is a Persistent Research Workflow Problem
Population gap detection is a critical but often underresourced step in research planning. Evidence from a 2022 National Academies report on clinical trial representation shows that even when clinical trials include underrepresented populations, subgroup-specific analyses are often missing or poorly executed — and that substantial underrepresentation persists particularly in oncology, cardiology, and Alzheimer's disease research. Population gap detection is one dimension of a broader research gap identification process; for a broader overview of how AI agent skills can support research gap analysis more generally, see How to Find Research Gaps in Medical Research Using AI Agent Skills.
What the Population Gap Detector Agent Skill Does
The Population Gap Detector is a AIPOCH agent skill designed specifically to help researchers identify evidence gaps by age, sex, geography, comorbidity, ancestry, or molecular subtype, so Researchers can target a more precise study population.
Input: A natural language query describing a disease area, biomarker, treatment context, or research direction where subgroup undercoverage is a concern. For example: "Which populations are under-studied in immunotherapy response biomarker research for lung cancer?"
Outputs: A structured Markdown report covering analytical sections:
- A precise definition of the topic unit
- A candidate population axes table across dimensions such as ancestry, sex, age, disease stage, molecular subtype, comorbidity, care setting, and geography
- A coverage audit of how the existing evidence base handles each subgroup axis
- A gap classification by type (Identify which subgroup gaps are present and what type of gap each represents.)
- A judgment on which gaps are meaningful versus cosmetic
- An evidence depth assessment by subgroup
- A priority ranking of the most defensible population gap for a next-step study
- A research translation framing, converting the selected gap into a more precise research direction.
- Risk Review
- References Researchers receive a starting point for researcher review; the skill does not replace expert scientific judgment or validate study design independently.
Workflow Execution Example: Immunotherapy Biomarker Research in NSCLC
The following workflow screenshots are illustrative diagrams for reference only.
Step 1 — Input
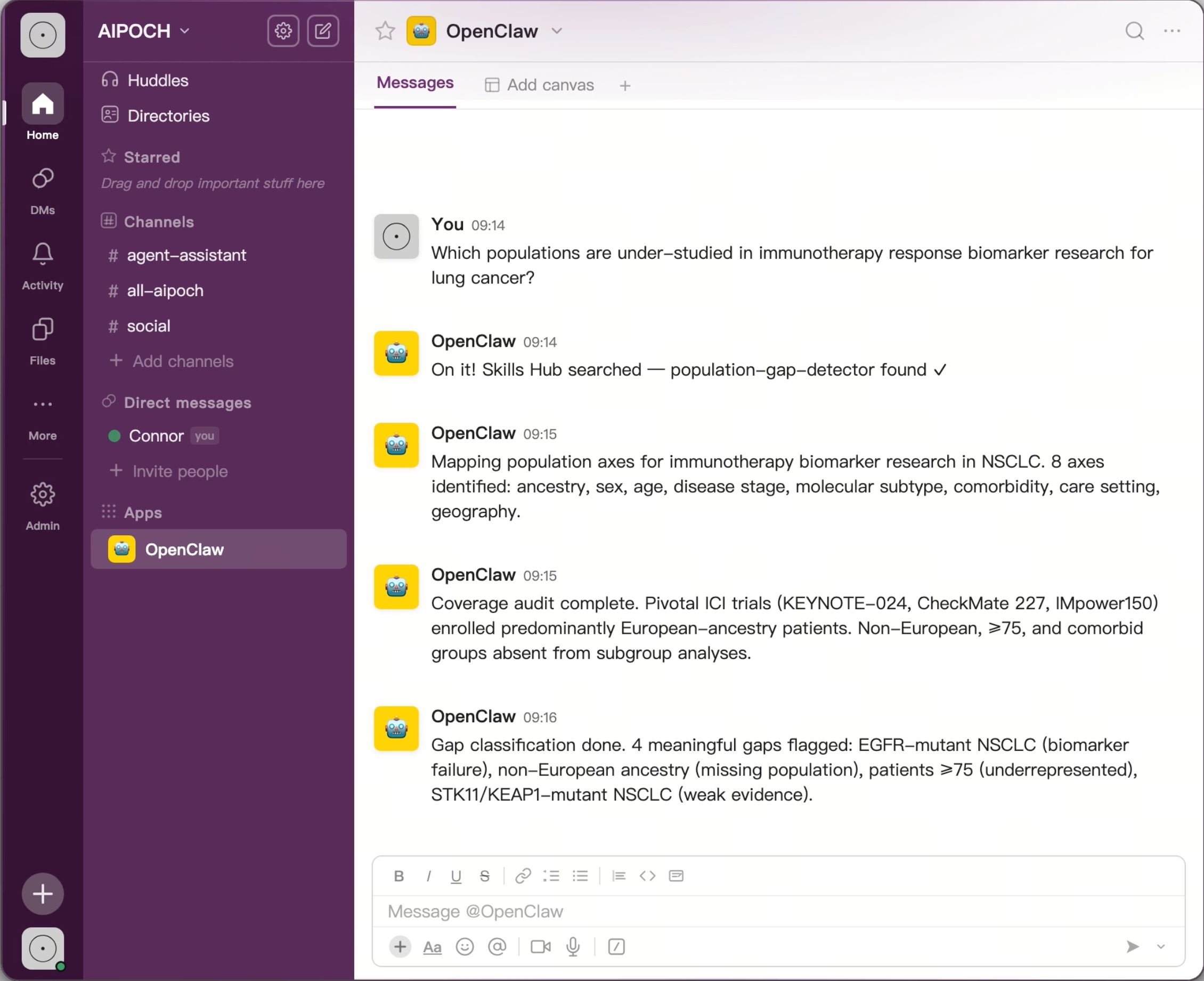
A researcher submits the question: "Which populations are under-studied in immunotherapy response biomarker research for lung cancer?"
The AI agent acknowledges the query, searches the skills hub for the appropriate skill, and confirms the Population Gap Detector has been selected.
Step 2 — AI Workflow Execution
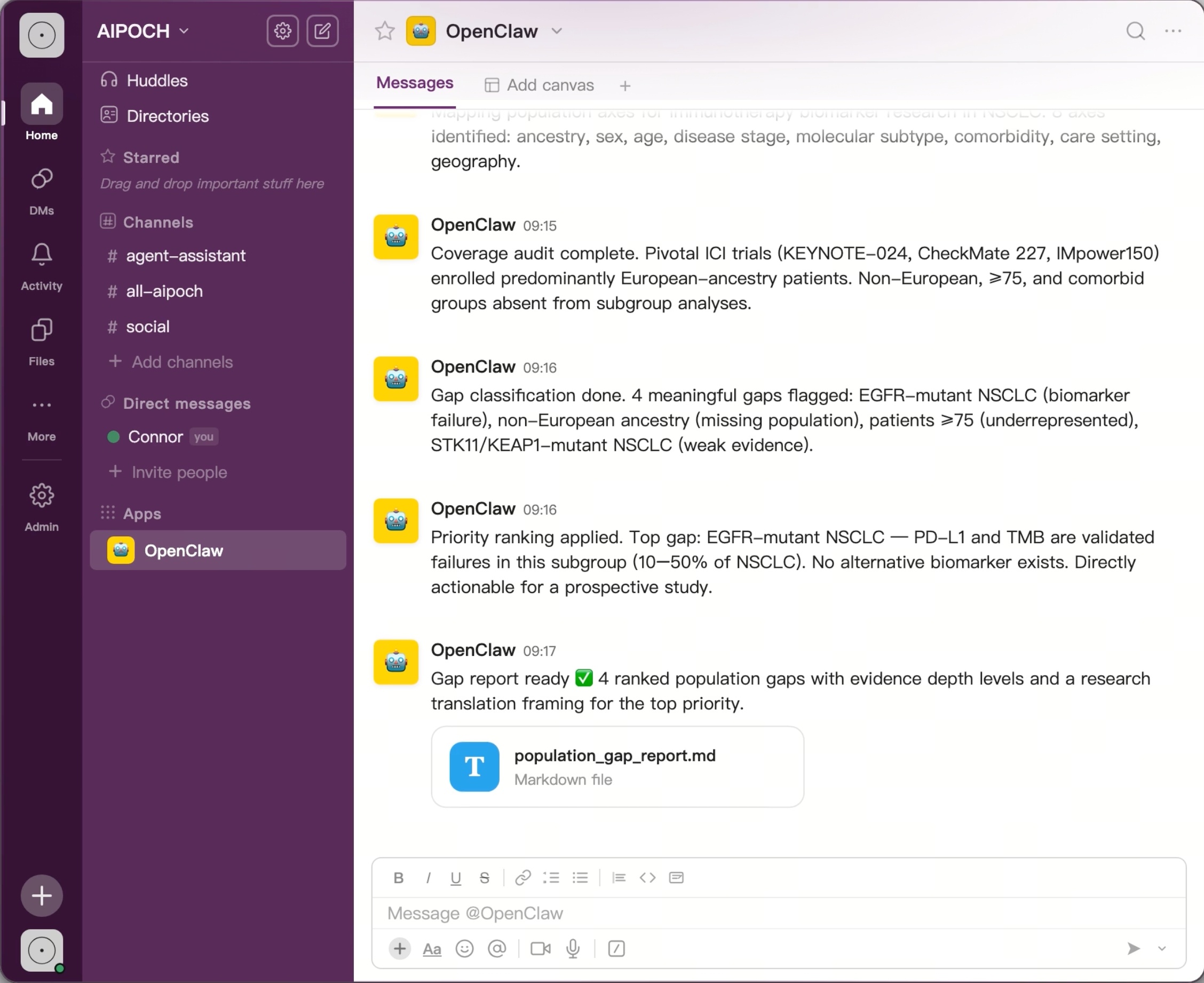
Once the skill is loaded, the agent proceeds automatically through the analysis. It maps 8 candidate population axes relevant to the topic, audits how well existing evidence covers each axis, classifies the gaps it finds, and applies a priority ranking to surface the most actionable one. In this example, 4 meaningful gaps are flagged and ranked.
Step 3 — Structured Outputs
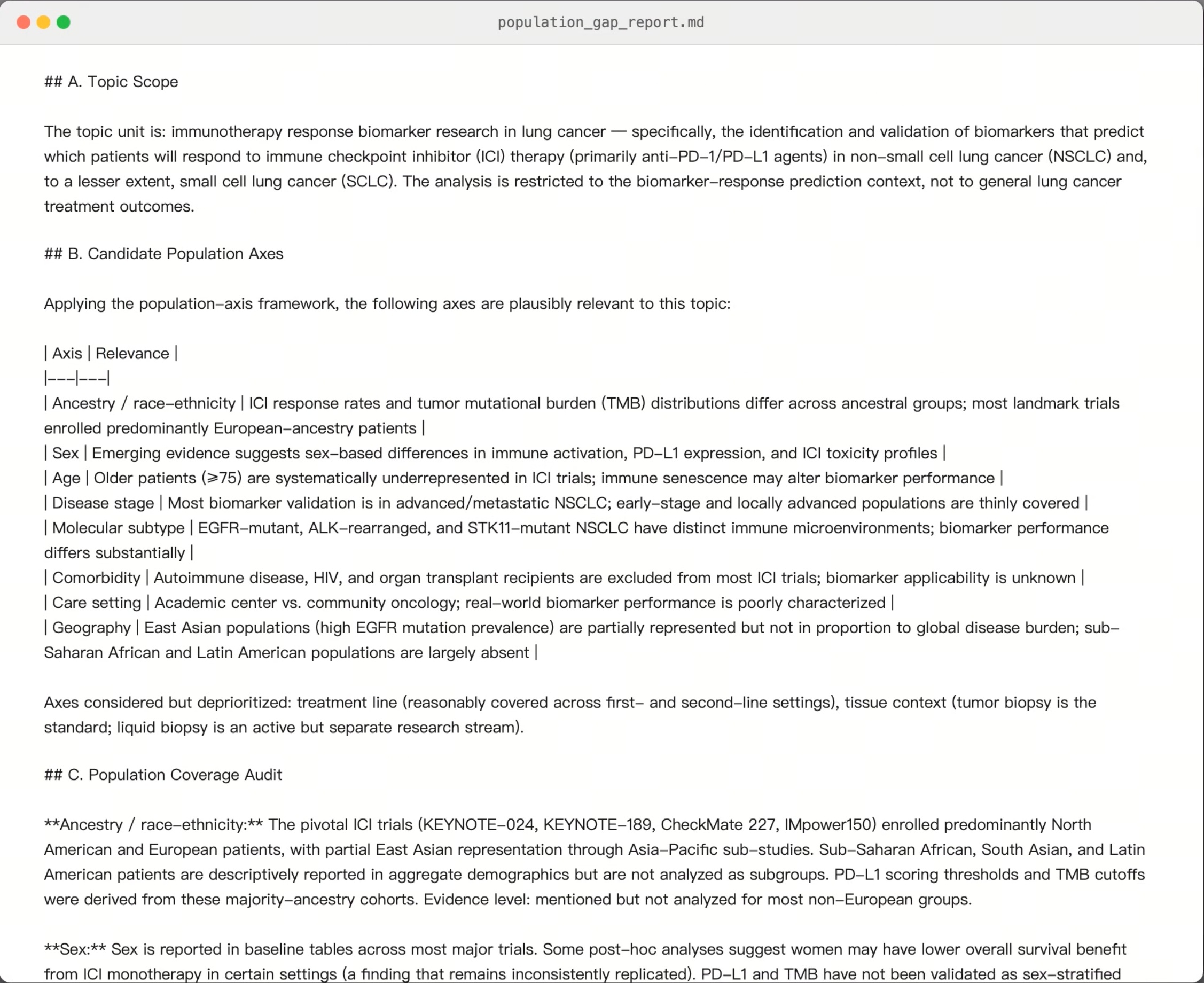
The skill produces a population_gap_report.md file organized across all mandatory output sections — from topic scope and candidate population axes through to a research translation framing.
When a population gap report suggests that subgroup underrepresentation is linked to methodological weaknesses — for example, when studies repeatedly exclude or under-analyze EGFR-mutant patients because of cohort design, sample size, or subgroup-analysis constraints — researchers may want to follow up with a methodological audit of the existing literature. AIPOCH’s Method Gap Detector is designed to support this next step by helping researchers identify design gaps, validation weaknesses, and reproducibility problems at the field level. See also: How to Identify Methodological Gaps in Research.
▶ Watch the demo: A full video walkthrough of this workflow is available below.
Example Research Use Cases
Oncology biomarker study population planning. A translational oncologist preparing a prospective biomarker study can use the Population Gap Detector to map which molecular subtypes and demographic groups are underrepresented in existing validation cohorts, can help researchers identify a study population that addresses a defensible evidence gap rather than repeating a well-covered research direction.
Systematic review scoping. A research team preparing a systematic review protocol can submit their topic to the skill to generate a population axis map and coverage audit as an input to their inclusion criteria design, reducing the risk of inadvertently excluding subgroup-specific evidence from the review scope. Researchers who want to map broader topic-level research gaps before narrowing to a population-specific question may also find the Medical Research Gap Finder useful as a prior step.
Conclusion
Population gap detection is a structured analytical task that sits between literature review and study design — too detailed for a general search, too complex for ad hoc judgment. The Population Gap Detector from AIPOCH is designed to help researchers organize and systematize this workflow step, producing a structured report that covers topic scoping, axis mapping, coverage auditing, gap classification, and research translation for researcher review. The skill supports the analytical judgment required for precise population-focused research — without replacing the expert interpretation that every study ultimately requires.
Once a priority population gap has been identified, researchers may want to assess whether pursuing that direction is both novel and practically achievable before committing resources. AIPOCH's Novelty vs Feasibility Assessor is designed to support this next-step evaluation, helping researchers decide whether to start, narrow, redesign, delay, or stop a proposed study direction.
AIPOCH is a collection of Medical Research Agent Skills designed to support AI-assisted biomedical research workflows across literature review, evidence organization, bioinformatics preprocessing, data analysis support, and research writing tasks. Explore the full skill library at the AIPOCH Agent Skills Library or browse the source repository at the AIPOCH GitHub — Medical Research Skills.
Frequently Asked Questions
What kind of input does the Population Gap Detector accept?
The skill accepts one or more of the following:
- a disease area with suspected heterogeneity
- a biomarker, treatment, mechanism, target, pathway, or phenotype plus a concern about subgroup undercoverage
- a research direction where representation, transportability, or subgroup specificity is uncertain
- a broad topic where the user wants to know which population is most overlooked
- a disease, endpoint, or use case where age, sex, geography, ancestry, comorbidity, disease stage, or molecular subtype may matter
How does the skill distinguish meaningful population gaps from cosmetic stratification?
The skill applies an explicit set of meaningful-versus-cosmetic stratification rules from its reference module library. A subgroup gap is treated as meaningful when it could plausibly affect disease biology, diagnosis, prognosis, treatment response, risk modeling, implementation, or the transportability of findings. A subgroup split is treated as cosmetic when it adds little biological, clinical, or interpretive value and mainly creates the appearance of precision. This judgment is documented in the output report for researcher review.
Can this skill replace a statistician or study design expert?
No. The Population Gap Detector produces structured outputs intended as a starting point for researcher review. It can help organize population axis mapping, coverage auditing, and gap classification — but all outputs require independent verification and expert interpretation before use in any research or clinical context. Study design, sample size estimation, and statistical planning remain the responsibility of qualified researchers and statisticians.
What output format does the skill produce?
The skill produces a structured Markdown report (population_gap_report.md) covering ten mandatory sections from topic scope through references. The report is designed to be reusable across team members and downstream tasks such as grant writing, systematic review scoping, and protocol development.
Disclaimer
This article is intended for informational purposes only and does not constitute medical advice, clinical guidance, diagnostic recommendations, treatment decisions, or validated scientific conclusions.
The skill does not replace researcher judgment. Researchers remain fully responsible for evaluating the accuracy, completeness, and appropriateness of any outputs generated. All outputs require independent verification and expert interpretation before use in any research or clinical context. The skill is not an approved medical device, clinical decision support system, or substitute for professional medical or scientific judgment.
References and external links in this article are provided for informational purposes. AIPOCH does not endorse and is not responsible for the content of third-party sources.